What is Minimally Invasive Thyroid Surgery?
Minimally invasive thyroid surgery is primarily defined by a reduced incision length in order to minimize postoperative pain, reduce length of hospital stay but most importantly, improve overall cosmetic results. These minimally invasive techniques were introduced within the past 15 years with the sole intention of surgically managing thyroid disease with minimal pain and complications.
The thyroid is located in the neck, below our larynx (voice box or “Adam’s apple”) and above the clavicles (collarbones) and surgery to this area for diseases associated with the gland can lead to large and very visible scars post operatively.
There are currently two approaches to minimally invasive surgery: 1) minimally invasive open thyroidectomy (MIT) and 2) minimally invasive video-assisted thyroidectomy (MIVAT).
MIT is similar to the conventional open thyroidectomy in its overall technique with the main difference being length of the neck incision which in order to be considered minimally invasive needs to be typically one that is less than 3 cm (1 inch). A smaller incision results in better overall cosmetic satisifaction and decreases patient discomfort. Thus other than the size of the cut made, there is no other technical difference between MIT and traditional open thyroid surgery.
MIVAT typically involves an incision no greater than 3cm (1 inch) and is placed slightly higher than the conventional thyroidectomy incision on the neck. Once the incision is made, the surgeon will then utilize endoscopic video-assisted techniques, which simply means he will place small cameras within the incision and use that to visualize the surgical field. With the advancements in fiber optics and surgical scopes, surgeons have been able to perform major surgeries without having to make large open incisions. This method also results in minimal blood loss and usually faster surgical speed resulting in less anesthesia exposure for the patient.
Dr. Parikh determines whether he will use an MIT or MIVAT or combination approach during surgery. He has experience doing several thousand of these procedures, arguably more than anyone else in the country.
Surgical Anatomy
The thyroid gland is located in the midline of the neck and is butterfly-shaped, about two inches in size and consisting of two lobes (i.e. the butterfly wings). Within the thyroid gland are also four small parathyroid glands, which play critical roles in our body’s calcium balance. Dr Parikh will preserve the parathyroid glands during thyroid surgery. The thyroid receives dual blood supply with one artery supplying blood to the top portion of the gland and another artery supplying the lower portion. The most critical component of this anatomy is the presence of the left and right recurrent laryngeal nerves which injury to this nerve is a well-defined risk of thyroid surgery. The right recurrent laryngeal nerve is more susceptible to injury however bilateral nerve damage can also occur. Because of this nerves close proximity to the thyroid gland, Dr Parikh performs laryngeal nerve monitoring throughout the thyroid surgery in order to avoid injury to the nerve. The nerve is responsible for motor function and sensation to the larynx (“voice box”) thus injury to this nerve can lead to hoarseness, impaired vocal register, loss of voice, difficulties swallowing or problems in the respiratory tract.
Reasons for Surgery
Your physician may decide that thyroid surgery is the best treatment option. Once it is determined that surgery is your best option, we recommend that you research the person that you have been referred to for surgery. General Surgeons and General ENT physicians often do a small number of thyroid surgeries every year.
At our center, Dr. Parikh performs between 10-15 thyroid surgeries per week. His practice is solely devoted to the treatment of thyroid and parathyroid disease.
What to Expect
Minimally invasive thyroidectomy is a procedure that very few surgeons perform on a daily basis. Surgery, in the hands of a competent surgeon, results in very good outcomes with minimal downtime. Most thyroid nodules, hyperthyroidism, goiters, and thyroid cancers can be treated with minimally invasive thyroid surgery. Each week, patients fly in from all over the country and even the world to have surgery with Dr. Parikh. Most patients arrive the day before surgery and fly or drive 24-48 hours after surgery. Our highly specialized trained nurses and staff deal with this surgery 10-15 times per week.
Conventional Thyroid Surgery
Post Operative Scar after 2 Weeks

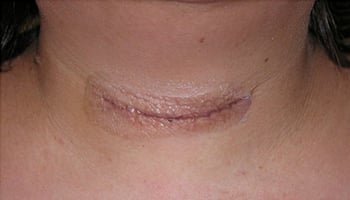
Dr. Shatul Parikh’s Minimally Invasive Thyroid Surgery
Post Operative Scar after 2 Weeks